Diabetic retinopathy affects an estimated 10 million Americans and remains a leading cause of preventable blindness among working-age adults. Despite evidence that up to 98% of severe vision loss from diabetes can be prevented through timely screening and intervention, adherence to annual dilated eye examinations has stagnated at approximately 50% for nearly two decades. This persistent screening gap reflects deep structural barriers: geographic maldistribution of eye care providers, workforce shortages in ophthalmology and optometry, and a referral-dependent care model that places the burden of access on patients who are often least equipped to navigate it. A series of articles from trusted physicians in the field examine the scope of the problem, and the emerging solutions poised to close this gap.
The Diabetic Retinopathy Screening Gap: Why Limited Access and Delayed Detection are Driving Preventable Vision Loss
Jonathan D. Agnew, PhD, MBA, Adjunct Professor, Faculty of Medicine, University of British Columbia
Burden and impact of diabetes and eye disease, screening adherence
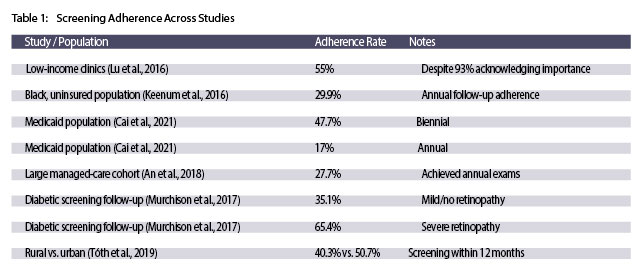
Diabetic retinopathy remains one of the most significant yet preventable causes of vision loss worldwide. Despite this preventability, screening rates have stagnated at approximately 50–60% for nearly two decades. This persistent gap between the availability of effective treatments and the failure to identify patients who need them represents a critical public health challenge requiring innovative solutions. Adherence data reveal a complex and concerning picture (Table 1) with the burden of diabetic eye disease falling disproportionately on underserved communities.
The consequences of inadequate screening extend beyond individuals to community and population-level outcomes. The low adherence rate has been established, but how does this impact outcomes, healthcare staff, or cost-effectiveness? When community screening programs are implemented, the diagnostic yield is substantial, with almost two thirds of diabetic patients having diagnosable eye conditions, and 40% showing diabetic retinopathy. (Cummings et al., 2001). The correlation between lower rural screening rates and higher blindness prevalence demonstrates the direct consequences of screening failure.
The evidence supporting early intervention is compelling. Pan-retinal laser photocoagulation reduces the risk of moderate and severe visual loss by 50% in patients with severe non-proliferative and proliferative retinopathy, while focal laser photocoagulation reduces moderate visual loss by 50–70% in eyes with macular edema. The Diabetic Retinopathy Study demonstrated that untreated eyes experienced a 15.9% rate of severe visual loss compared to 6.4% in treated eyes over two years. Early laser photocoagulation provides additional long-term protection against severe vision loss with only 2.6% of patients having severe vision loss with early treatment versus 3.7% with deferred treatment during a five-year period. These treatment benefits depend entirely on detecting disease before irreversible damage occurs. Treatment timing directly affects outcomes. A study of patients with proliferative diabetic retinopathy found that those treated more than 31 days after diagnosis experienced significantly worse visual acuity at both 12 months and 24 months compared to those treated on the day of diagnosis. The average time for treatment was 27.8 days, with substantial variation suggesting many patients experience delays that compromise their visual outcomes. Among patients with retinopathy requiring treatment, the annual incidence of blindness ranges from 6% to 9%. These findings emphasize that screening programs must not only identify disease but increase access and time to treatment.
How Limited Access to Eye Screening Services Impacts Patients with Diabetes: Challenges and Emerging Solutions
Grayson W Armstrong, MD, MPH, Massachusetts Eye & Ear at Harvard Medical School
Scalability, cost effectiveness, preventing vision loss.
The rising prevalence of diabetes poses a challenge to healthcare systems and poses a significant risk for worsening rates of preventable vision loss from diabetic eye disease. The number of eye care providers isn’t growing at a fast enough rate to keep up with serving an aging population and growing prevalence of diabetes. Combined with infrastructure limitations and access disparities, this gap underscores the urgent need for innovative solutions. AI-driven screening tools and telemedicine offer scalable, cost-effective alternatives that expand access and improve outcomes. By leveraging these advancements and implementing supportive policies, healthcare systems can bridge the gap in diabetic eye screening and ensure that no patients’ vision is lost to a preventable disease.
Handheld retinal imaging devices like the Optomed Aurora camera enable high-quality fundus photography in primary care settings, mobile care units, or patient homes. Images can be analyzed by AI algorithms or transmitted to remote eye care specialists for interpretation. Additionally, ophthalmic telemedicine platforms allow for seamless integration of screening into existing healthcare workflows, particularly in remote, rural, and underserved areas. These innovations reduce detection delays, increase patient convenience, and eliminate logistical barriers to traditional screening visits.
AI and telemedicine improve accessibility and reduce costs by scaling more rapidly than traditional programs while requiring minimal training for non-specialist healthcare workers. Getting non-specialist healthcare workers involved in the screening workflow frees up ophthalmologists and optometrists to do more impactful treatment and management of patients. Handheld cameras are portable, accessible for patients with mobility issues, and highly effective in detecting diabetic retinopathy. Integrated AI systems like AEYE-DS deliver rapid, portable screening at the point of care.
Portable AI Screening at the Point of Care: Transforming Diabetic Retinopathy Detection, Access, and Ophthalmology Workflows
Jonathan D. Agnew, PhD, MBA, Adjunct Professor, Faculty of Medicine, University of British Columbia
Clinical validation and real-world results.
Clinical validation of AI DR screening systems in clinical practice demonstrates exceptional diagnostic performance. Two studies report 100% sensitivity for detecting referable diabetic retinopathy, ensuring at-risk patients receive appropriate specialist evaluation. Technical success rates exceed 89%, with the primary limitation being small pupils and patient refusal of dilating drops.
Implementation studies reveal a striking improvement in patient follow-up with specialist care when AI screening is integrated into primary care. AI screening has increased follow-up compliance by 13 to 57 percentage points. One particularly notable study demonstrated that follow-up compliance nearly tripled—from 18.7% to 55.4%—when AI screening was implemented. The speed of result delivery directly correlates with improved follow-up rates. Studies that reduced result turnaround from days to under an hour showed the largest compliance gain. Real-world implementation data show meaningful increases in overall screening rates. AI integration has improved screening completion by 25–30% and follow-up rates by approximately 15% among patients with significant retinopathy. By reducing unnecessary specialist referrals while ensuring appropriate engagement for high-risk patients, AI screening allows specialists to allocate their limited capacity more efficiently. This targeted approach enables specialist clinics to focus on patients who genuinely require intervention, improving both access to care and clinical outcomes.
Economic analyses consistently favor point-of-care AI screening. Seven of eight cost-effectiveness studies demonstrated AI-based screening as cost-effective or cost-saving when compared to traditional methods. Australian modeling projected universal AI screening could prevent over 38,000 blindness cases while saving AU$595.8 million over 40 years. Point-of-care programs achieve 35–64% cost reductions compared to specialist-delivered screening, with semi-automated approaches reducing costs by approximately 20%. Patient acceptance is also consistently high (96% satisfaction, average score 4.8/5). Eighty-one percent of patients prefer AI-based screening at primary care locations over separate specialist appointments, and immediate results facilitate meaningful patient education. This suggests possible hidden economic benefits of patient choice and improved adherence, as greater convenience and immediate feedback encourage follow-through with recommended care while reducing downstream costs associated with delayed diagnosis and treatment.
The Importance of Early Detection – How Patients with Diabetes can Significantly Reduce Their Risk of Blindness with Early Diagnosis and Treatment
Mohammad Rafieetary, OD, FAAO, FORS, ABO, Charles Retina Institute
Screening and Diagnosis
Early-stage diabetic retinopathy (mild to moderate) progresses slowly, often with no symptoms. However, once it advances to moderately severe or severe stages, progression accelerates and visual symptoms may emerge. Structural damage becomes irreversible, leading to permanent vision loss. Early detection and management are critical to preventing blindness. Key barriers to detection include lack of disease awareness, absence of symptoms, limited access to screening, transportation challenges, inadequate insurance, burdensome follow-up requirements, and poor patient-provider communication. Patient education, improved doctor-patient relationships, and accessible screening options with reduced office visit burden increase adherence.
Fundus photography has evolved dramatically with digital imaging, providing instant, high-resolution images. Recent advances combining user-friendly handheld devices with AI-assisted interpretation create a powerful tool for capturing at-risk patients. The Optomed Aurora AEYE, FDA-cleared with embedded AI, detects diabetic retinopathy with high sensitivity and specificity across diverse settings. Telemedicine advancements enable remote retinal imaging combined with AI interpretation, allowing primary care physicians to identify and refer DR patients without in-person ophthalmology visits. This approach is particularly effective in rural and underserved areas, reducing burden on specialized facilities while enabling integrated diabetes management through cloud-based platforms.
Overcoming Patient Backlogs in Ophthalmology Care: The Impact of Point-of-Care Screening on Diabetic Retinopathy Management
Blake Cooper, MD, MPH, FACS, Retina Associates Kansas City
Real world impact of AI DR screening
Diabetic retinopathy remains a growing public health crisis. Over 14% of the U.S. population has diabetes; approximately 26% develop some form of DR, with 5% progressing to vision-threatening disease. Despite being treatable when detected early, DR screening rates remain unacceptably low due to asymptomatic early disease, limited eye care professionals, work disruptions, cost, and complexity of traditional screening.
AI-assisted retinal cameras in primary care settings enhance DR screening rates and improve follow-up for serious retinopathy. In real world cases, AI-assisted screening for diabetes increased screening rates by 30% over five months in one large metropolitan district and 25% increase in a network of community health centers. Patient education and counseling about risk of potential vision loss from untreated DR leads to higher rates of patient adherence to referrals. This approach addresses delayed diagnoses and patient backlogs while increasing screening efficiency and accessibility.
Integrated point-of-care systems using handheld retinal imaging with embedded AI overcome screening barriers while facilitating patient education and management. Implementing these technologies in routine primary care settings is essential for improving DR screening rates, optimizing resource utilization, and patient outcomes.
Improving Patient Access to Screening – How Portable Screening Technologies are Helping to Detect Patients at the Point-of-Care (in-clinic or at home) and Prevent Unnecessary Ophthalmology Referrals
Carolyn Majcher, OD, FAAO, FORS, Northeastern State University Oklahoma College of Optometry
Demand for screening in ophthalmology
Diabetes prevalence has reached epidemic levels. The CDC reports 38.4 million Americans have diabetes (12% of the population). Diabetic retinopathy is the leading cause of blindness in working-aged Americans, affecting approximately 30% of adults with diabetes. Globally, DR prevalence among those with diabetes was 22.3% in 2020 (103.12 million people), with 6% having vision-threatening DR and 4% having clinically significant macular edema. By 2045, these numbers are projected to increase to 160.5 million, 44.8 million, and 28.6 million respectively. The American Diabetes Association (ADA) and the American Optometric Association recommend an eye exam 5 years after diagnosis for patients with type 1 diabetes and at least annually thereafter. Those with type 2 diabetes should be evaluated at time of diagnosis since diabetes may have gone undetected for years prior making it challenging to determine the exact duration of the disease. Despite these recommendations, DR screening rates have stagnated at 50% for approximately the past 20 years.
The ophthalmology workforce is projected to decline by 12% (2,650 full-time equivalents) by 2035, with rural areas disproportionately affected. Although DR rates are similar in rural and non-rural populations, rural areas show higher blindness rates due to lower screening and treatment rates.
Portable AI systems and telemedicine supplement traditional clinic-based assessment, enabling widespread screening especially in rural areas. Remote screening through primary care and endocrinology offices consolidates appointments, reducing time burden. AI systems provide diagnostic guidance, enabling non-eye care providers to utilize screening devices. Handheld Aurora AEYE is particularly valuable for patients with mobility restrictions.
How a Portable AI Screening Tool Like Aurora AEYE Can Enable Immediate, On-The-Spot Detection of Diabetic Retinopathy and Help Prevent Diabetes-Related Blindness
Steven Ferrucci, OD, FAAO, Sepulveda VA Medical Center
Community-based screening
Cost effective and efficient screening programs to detect diabetic retinopathy, especially those cases requiring treatment, are essential. This is especially true as diabetes prevalence increases. Community-based tele-retinal screening programs place non-mydriatic fundus cameras in community health centers where patients have retinal photos taken and remotely analyzed by trained readers. Results guide follow-up, referral, and treatment recommendations, reducing the need for in-person eye exams while demonstrating cost-effectiveness and efficacy.
However, traditional programs face barriers: high equipment cost, training expenses, and geographic/transportation challenges. Portable handheld equipment offers an attractive alternative with lower cost, greater accessibility, and improved portability. AI systems have proven effective in lowering costs, improving diagnostic accuracy, and increasing patient access. Those that provide immediate results eliminate the delay in obtaining results, leading to more timely referrals, compliance, and treatment if required. These systems limit the amount of unnecessary referrals and optimize patient and provider burden. The first FDA-cleared AI medical device for diabetic retinopathy detection was approved in April 2018, with only a single one approved for use on a handheld device. AI-based deep learning excels in image processing and computer-aided diagnostics, with accuracy comparable to expert screenings across ophthalmology, dermatology, radiology, and gastroenterology.
Future Outlook: Emerging Trends and Technologies in Diabetic Retinopathy Screening
Jonathan D. Agnew, PhD, MBA, Adjunct Professor, Faculty of Medicine, University of British Columbia
Screening for Systemic Disease Through Retinal Imaging
AI systems have evolved from single-disease detection to comprehensive multi-disease platforms simultaneously screening for diabetic retinopathy, glaucoma, and age-related macular degeneration. “Oculomics” is an emerging field analyzing retinal images for systemic disease. It leverages the retina as the only site where microvasculature can be directly imaged non-invasively.
For diabetic patients at elevated cardiovascular, kidney disease, and Alzheimer’s disease risk, AI analysis detects early microvascular biomarkers in retinal images that precede clinical symptoms. Retinal features associated with cardiovascular disease risk, chronic kidney disease progression, and neurodegenerative conditions can be identified through standard fundus photography.
Predictive analytics now forecast diabetic retinopathy progression over two-year horizons, identifying high-risk patients for proactive intervention. A single retinal image at a primary care visit could yield actionable insights across multiple disease domains. Cardiovascular risk prediction from retinal images achieves accuracy comparable to established risk calculators. For diabetic patients with two to four times higher cardiovascular risk, this enables opportunistic cardiovascular assessment during retinopathy screening without additional procedures or cost.
Chronic kidney disease, affecting approximately 40% of diabetic individuals, can be identified early through AI analysis of retinal microvascular features, enabling earlier nephrology referral and intervention. Retinal biomarkers associated with Alzheimer’s disease may precede cognitive symptoms by years.
As oculomics algorithms receive regulatory clearance, handheld fundus cameras will evolve from diabetic retinopathy screeners into comprehensive systemic health screening tools, multiplying the clinical value of each point-of-care encounter.
Share this insight
